Über 300.000 Menschen erleiden in Deutschland jedes Jahr einen Herzinfarkt. Wie hoch Ihr eigenes Risiko für dieses meist dramatische Ereignis ist, zeigt Ihnen der Online-Test der Deutschen Herzstiftung.
Kardiovaskuläres Risiko bei chronischer metabolischer Azidose
Die teilweise dramatischen Zusammenhänge zwischen Herz-Kreislauf-Erkrankungen und chronischer Übersäuerung können Sie in dem folgenden Video sehen. Hier haben wir eine aktuelle Studie ausgewertet, die das Risiko für kardiovaskuläre Ereignisse, wie z. B. Herzinfarkt, Schlaganfall, Herzinsuffizienz und Tod, genau quantifiziert und damit die dringende Behandlungsbedürftigkeit einer Azidose untermauert.
Die
Niere
spielt eine entscheidende Rolle bei der Aufrechterhaltung des Säure-Base-Gleichgewichts. Bei einer chronischen
Niereninsuffizienz
(CKD) ist die Fähigkeit der
Niere,
Säuren auszuscheiden und Bikarbonat zum systemischen Säureausgleich zu reabsorbieren, beeinträchtigt. Demzufolge ist eine
chronische metabolische Azidose
(cmA) mit Serum-Bikarbonat-Spiegeln (TCO2) unter 22 mmol/L bei CKD besonders häufig.
Arterielle Steifigkeit ist bei Nierenschwäche häufig und entsteht durch mediale Kalzifizierungen von elastischen Arterien. Sie wird als Surrogatmarker für
Arteriosklerose
verwendet
[3] und ist ein Risikofaktor für kardiovaskuläre Ereignisse [4, 6]. Die Pulswellengeschwindigkeit (PWV) ist ein physiologischer Standard-Parameter zur Bewertung der vaskulären Steifigkeit [5] und beschreibt die Geschwindigkeit, mit der die durch Kontraktion des
Herzens
erzeugte Blut-Druckwelle das
arterielle Gefäßsystem
durchläuft. Je steifer die
Arterienwand,
desto schneller ist die Pulswelle. Die am häufigsten verwendeten PWV sind die karotisch-femorale (cfPWV; ein Maß für die Aortensteifigkeit) und die Arm-Knöchel-PWV (baPWV; ein Maß für die zentrale und periphere arterielle Steifigkeit).
Chronische Azidose
ist mit
Arteriosklerose
assoziiert
In einer früheren Studie konnten bei Hämodialyse-Patienten Veränderungen der Pulswellengeschwindigkeit im Zusammenhang mit Serum-Bikarbonat-Konzentrationen beobachtet werden: Die Gruppe mit den niedrigsten Bikarbonat-Spiegeln (TCO2 < 20 mmol/L) zeigte signifikant größere PWV-Zunahmen über den 1-Jahres-Studienzeitraum [7]. In einer anderen Studie waren die Bikarbonat-Spiegel bei Hämodialyse-Patienten invers mit der cfPWV assoziiert (p = 0,001) [8]. Oka et al. konnten zeigen, dass niedrige Bikarbonat-Spiegel während der Prädialyse-Phase bei Dialyse-Patienten das Risiko für
Koronar-Arterien-Kalzifikationen
erhöhen [9].
Diese Beobachtungen legen nahe, dass bei Hämodialyse-Patienten eine
chronische metabolische Azidose,
arterielle Steifheit und
Arteriosklerose (Atherosklerose)
eng miteinander verbunden sind. Um zu prüfen, ob dies auch auf prädialytische Stadien der
Niereninsuffizienz
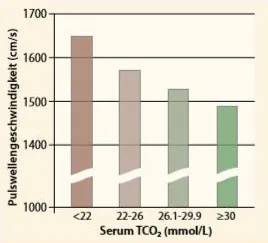
Die Pulswellengeschwindigkeit war bei einer chronischen Azidose signifikant höher als bei den Kontroll-Gruppen. Quelle: [2].
zutrifft, wurden 1.659 CKD-Patienten in eine klinische Studie eingeschlossen [2]. Prüfparameter waren Serum-Bikarbonat-Spiegel und baPWV.
Insgesamt wurden bei 12,7 % der niereninsuffizienten Patienten eine chronische Übersäuerung diagnostiziert (TCO2 < 22 mmol/L); im Stadium 4 hatten 26 % und im Stadium 5 hatten 47,4 % eine cmA. Je weiter fortgeschritten die CKD, desto niedriger waren die Bikarbonat-Spiegel (p < 0.001). Die baPWV war bei Patienten mit
chronisch metabolischer Azidose
signifikant höher (p < 0,001) und zeigte eine inverse Korrelation mit dem Serum-Bikarbonat (s. Diagramm). Diese Daten zeigen, dass bereits in der Prädialyse bei einer
chronischen metabolischen Azidose,
die Arteriensteifigkeit und damit das Risiko für vaskuläre Kalzifikationen steigt.
Pathomechanismen
Eine cmA induziert verschiedene negative Mechanismen, die zu einer
Arteriosklerose
beitragen können [3, 10]. Dazu zählen:
Knochenresorption mit Anstieg der Kalzium- und Phosphat-Ionen im Serum
arterielle Inflammationen mit Freisetzung von Zytokinen
Insulinresistenz / Beeinträchtigung der Glukosetoleranz
Abbau von Muskelproteinen,
Muskelschwund,
Fazit: Eine behandlungsbedürftige
chronische metabolische Azidose
wird häufig schon in der Prädialyse beobachtet und forciert u.a. die Progression einer
Niereninsuffizienz,
verschlechtert die Arteriensteifigkeit und erhöht das Risiko für
Arteriosklerose
und kardiovaskuläre Ereignisse. Therapeutisch kann eine cmA effektiv mit 2-3g/d Natriumbikarbonat behandelt werden und die Pufferreserven wieder auffüllen. Dabei ist allerdings eine magensaftresistente Formulierung entscheidend für eine gute Wirksamkeit und den Therapieerfolg.
Wissen
Mehr zum Sterberisiko bei chronischer metabolischer Azidose können Sie in der folgenden wissenschaftlichen Ausarbeitung lesen. Hier haben wir eine aktuelle Studie ausgewertet, die das Risiko für kardiovaskuläre Ereignisse, wie z. B. Herzinfarkt, Schlaganfall, Herzinsuffizienz, genau quantifiziert.
The kidney has the principal role in the maintenance of acid-base balance. Therefore, a decrease in renal ammonium excretion and a positive acid balance often leading to a reduction in serum bicarbonate concentration are observed in the course of chronic kidney disease (CKD). The decrease in serum bicarbonate concentration is usually absent until glomerular filtration rate decreases
to <20 to 25mL/min/1.73 m(2), although it can develop with lesser degrees of decreased kidney function. Non-anion gap acidosis, high-anion gap acidosis, or both can be found at all stages of CKD. The acidosis can be associated with muscle wasting, bone disease, hypoalbuminemia, inflammation, progression of CKD, and increased mortality.
Administration of base may decrease muscle wasting, improve bone disease, and slow the progression of CKD. Base is suggested when serum bicarbonate concentration is <22 mEq/L, but the target serum bicarbonate concentration is unclear.
Evidence that increments in serum bicarbonate concentration > 24 mEq/L might be associated with worsening of cardiovascular disease adds complexity to treatment decisions. Further study of the mechanisms through which metabolic acidosis contributes to the progression of CKD, as well as the pathways involved in mediating the benefits and complications of base therapy, is warranted.
Abstract: Metabolic acidosis is associated with pulse wave velocity in chronic kidney disease: Results from the KNOW-CKD Study.
Metabolic acidosis is common in chronic kidney disease (CKD) and may have various deleterious consequences. Arterial stiffness in CKD patients is associated with poor cardiovascular outcomes. The present study aimed to evaluate the association between serum bicarbonate and arterial stiffness using the baseline cross-sectional data set of a large-scale Korean CKD cohort. 2,238 CKD patients were enrolled in the KoreaN Cohort Study for Outcome in Patients With Chronic Kidney Disease (KNOW-CKD) from 2011 to 2016. The present study was conducted on 1,659 patients included in this cohort with baseline serum bicarbonate and brachial-to-ankle pulse wave velocity (baPWV) data. Metabolic acidosis was defined as a serum bicarbonate level of <22 mmol/L, and baPWV was used as a surrogate of arterial stiffness. Mean serum bicarbonate was 25.8 ± 3.6 mmol/L. 210 (12.7%) patients had metabolic acidosis. baPWV was significantly higher in patients with metabolic acidosis (P < 0.001) and showed a significant inverse correlation with serum bicarbonate (Unstandardized β -16.0 cm/sec; 95% CI -20.5, -11.4; P < 0.001) in an unadjusted model, which was retained after adjustment (Unstandardized β -5.4 cm/sec; 95% CI -9.9, -1.0; P = 0.017). Metabolic acidosis was found to be associated with a high baPWV in pre-dialysis CKD patients.
Abstract: Arterial Stiffening and Clinical Outcomes in Dialysis Patients.
Cardiovascular disease (CVD) is an important cause of morbidity and mortality in dialysis patients. Brachial-ankle pulse wave velocity (baPWV) is more efficient to handily assess arteriosclerosis than aortic PWV. The cardio-ankle vascular index (CAVI) is also a novel blood pressure-independent arterial stiffness parameter. In dialysis patients, both baPWV and CAVI are increased compared to general subjects. Several studies have demonstrated that increased baPWV is associated with carotid atherosclerosis and diastolic left ventricular dysfunction in hemodialysis (HD) patients. In addition, higher baPWV is related to all-cause and cardiovascular (CV) mortality. CAVI is similarly associated with CVD. However, baPWV is superior to CAVI as a predictor of CV outcomes in HD patients. Besides these outcomes, a close relationship exists between sarcopenia, abdominal visceral obesity and arterial stiffening. Reduction of thigh muscle mass is inversely correlated with baPWV and CAVI in males. Abdominal fatness is also associated with increased arterial stiffness in females. These observations provide further evidence of higher risk of CV events in HD patients with sarcopenic obesity. In addition, arterial stiffness is associated with cerebral small vessel disease and decreased cognitive function in the elderly. However, it is unknown whether arterial stiffness may be useful as an early indicator of cognitive decline in dialysis patients. Because dialysis patients are at risk of developing dementia, more studies are needed to elucidate the causal link between arterial stiffness and cognitive impairment.
Abstract: Arterial Stiffness and Chronic Kidney Disease.
Chronic kidney disease (CKD) is a major public health concern due to the high prevalence of associated cardiovascular (CV) disease. CV mortality is 10-30 times higher in end-stage renal disease patients than in the age-adjusted general population. The last 20 years have been marked by a huge effort in the characterization of the vascular remodeling process associated with CKD and its consequences on the renal, CV and general prognosis. By comparison with patients with normal renal function, with or without hypertension, an increase in large artery stiffness has been described in end-stage renal disease as well as in CKD stages 2-5. Most clinical studies are consistent with the observation that damage to large arteries may contribute to the high incidence of CV disease. By contrast, the impact of large artery stiffening and remodeling on CKD progression is still a matter of debate. Concomitant exposure to other CV risk factors, including diabetes, seems to play a major role in the association between aortic stiffness and estimated GFR. The conflicting results obtained from longitudinal studies designed to evaluate the impact of baseline aortic stiffness on GFR progression are detailed in the present review. Only pulse pressure, central and peripheral, is almost constantly associated with incident CKD and GFR decline. Kidney transplantation improves patients' CV prognosis, but its impact on arterial stiffness is still controversial. Donor age, living kidney donation and mean blood pressure appear to be the main determinants of improvement in aortic stiffness after kidney transplantation.
Abstract: Validity, reproducibility, and clinical significance of noninvasive brachial-ankle pulse wave velocity measurement.
The present study was conducted to evaluate the validity and reproducibility of noninvasive brachial-ankle pulse wave velocity (baPWV) measurements and to examine the alteration of baPWV in patients with coronary artery disease (CAD). Simultaneous recordings of baPWV by a simple, noninvasive method and aortic pulse wave velosity (PWV) using a catheter tip with pressure manometer were performed in 41 patients with CAD, vasospastic angina, or cardiomyopathy. In 32 subjects (15 controls and 17 patients with CAD), baPWV was recorded independently by two observers in a random manner. In 55 subjects (14 controls and 41 patients with CAD), baPWV was recorded twice by a single observer on different days. baPWV were compared among 172 patients with CAD (aged 62 +/- 8 years); 655 age-matched patients without CAD but with hypertension, diabetes mellitus, or dyslipidemia; and 595 age-matched healthy subjects without these risk factors. baPWV correlated well with aortic PWV (r=0.87, p<0.01). Pearson's correlation coefficients of interobserver and intraobserver reproducibility were r=0.98 and r=0.87, respectively. The corresponding coefficients of variation were 8.4% and 10.0%. baPWV were significantly higher in CAD patients than in non-CAD patients with risk factors, for both genders (p<0.01). In addition, baPWV were higher in non-CAD patients with risk factors than in healthy subjects without risk factors. Thus, the validity and reproducibility of baPWV measurements are considerably high, and this method seems to be an acceptable marker reflecting vascular damages. baPWV measured by this simple, noninvasive method is suitable for screening vascular damages in a large population.
Abstract: Comparison between carotid-femoral and brachial-ankle pulse wave velocity as measures of arterial stiffness.
BACKGROUND: Arterial stiffness is an important risk factor for cardiovascular disease. Carotid-femoral pulse wave velocity (cfPWV) is the most recognized and established index of arterial stiffness. An emerging automatic measure of PWV primarily used in the Asian countries is brachial-ankle PWV (baPWV). METHODS: To systematically compare these two methodologies, we conducted a multicenter study involving a total of 2287 patients. RESULTS: There was a significant positive relation between baPWV and cfPWV (r = 0.73). Average baPWV was approximately 20% higher than cfPWV. Both cfPWV and baPWV were significantly and positively associated with age (r = 0.56 and 0.64), systolic blood pressure (r = 0.49 and 0.61), and the Framingham risk score (r = 0.48 and 0.63). The areas under the receiver operating curves (ROCs) of PWV to predict the presence of both stroke and coronary artery disease were comparable between cfPWV and baPWV. CONCLUSIONS: Collectively, these results indicate that cfPWV and baPWV are indices of arterial stiffness that exhibit similar extent of associations with cardiovascular disease risk factors and clinical events.
Abstract: The role of oral sodium bicarbonate supplementation in maintaining acid-base balance and its influence on the cardiovascular system in chronic hemodialysis patients - results of a prospective study.
BACKGROUND: Major acid-base variations during dialysis and the imbalances in serum calcium levels intensified by them play a role in cardiovascular damage of hemodialysis patients. Early vascular walls modifications can be objectified by determining the pulse wave velocity (PWV) - a marker of vascular stiffness that is associated with increased risk of cardiovascular events. Material and methods: This was a prospective study conducted on 63 chronic hemodialysis patients with diuresis above 500 mL/ 24 hours and predialysis blood pressure below 160 mmHg (treatment controlled) randomized in two groups for 12 months - the study group receiving interdialitic oral sodium bicarbonate doses and control group, without oral sodium bicarbonate supplementation, but receiving higher bicarbonate prescriptions in dialysis. All the patients were monthly evaluated by biochemical tests (serum calcium, phosphate, iPTH, bicarbonate), the assessment of prescribed doses of phosphate binders being undergone. Two PWV determinations and chest X-ray exams for coronary calcifications were done - at the beginning and end of the study for every patient. RESULTS: In the study group (n = 29), the mean age was 56.48 ± 12.78 years and the average duration of dialysis was 55.51 ± 34.53 months, the mean dialysis bicarbonate was 29.81 ± 1.41 mEq/ L and 27 of them (subgroup 0) had alkaline reserve (AR) 20-22 mEq/ L. The control group (n = 34) had a mean age of 57.35 ± 15.32 years and the mean dialysis duration 59.67 ± 34.79 months, with an average level of dialysis bicarbonate of 33 ± 2.2 mEq/ L necessary to maintain AR within guidelines. Depending on the mean AR obtained, this group was divided into three subgroups (subgroup 1, subgroup 2, and subgroup 3). There were statistically significant differences regarding the necessary of dialysis bicarbonate (p < 0.001), average serum calcium levels (p < 0.001) and serum phosphorus (p < 0.001), as well as PWV mean values and the number of vascular calcifications (p = 0.036) between the study and the control group. The average dose of phosphate binders was significantly higher in the study group (p = 0.01). At the end of the study, the serum iPTH average levels were decreased in the study group (p < 0.001) and significantly increased in the control group (p < 0.001). CONCLUSIONS: Avoiding large variations in serum bicarbonate levels is an important step in hemodialysis patients' management because wide acidosis-alkalosis variation can increase cardiovascular risks in terms of altering the vessel walls elasticity and favoring their calcifications. ABBREVIATIONS: GFR = glomerular filtration rate,PWV = pulse wave velocity, iPTH = intact parathyroid hormone,AR = alkaline reserve, BP = blood pressure,mEq = milliequivalents,L = liter.
KEYWORDS:arterial stiffness; bone mineral disease; hemodialysis; sodium bicarbonate
Published by Journal of Medicine and Life.PMID: 27928454
Abstract: β2-Microglobulin, pulse pressure and metabolic alterations in hemodialysis patients.
BACKGROUND:Pulse pressure (PP) is a result of arterial stiffness seen in dialysis patients, but may be a consequence of fluid overload. We examined the role of β(2)-microglobulin (β(2)M) in PP in relation to metabolic alterations in patients on different hemodialysis (HD) modalities. METHODS: We studied 76 hemodialyzed patients on regular HD (n = 34), predilution bagged hemodiafiltration (n = 19) and online predilution hemodiafiltration (n = 23). β(2)M levels were measured by radioimmunoassay, and the clearance of β(2)M was assessed by Kt/V for β(2)M. Arterial stiffness was measured as carotid-femoral pulse wave velocity, and PP was derived. Insulin levels were measured using immunoradioassay, and insulin resistance was calculated using homeostasis model assessment insulin resistance (HOMA-IR). Serum bicarbonate levels were measured using a blood gas analyzer, and percent sodium removal was calculated. RESULTS: β(2)M levels predict increased PP (p = 0.02) adjusting for age, HD modalities, HD duration, HOMA-IR and percent sodium removal. β(2)M was positively associated with HOMA-IR (r = 0.306, p = 0.007). Serum bicarbonate levels and carotid-femoral pulse wave velocity were inversely associated (r = -0.719, p = 0.001). CONCLUSIONS: β(2)M levels were positively associated with PP, which was influenced mainly by dialysis modality fluid and sodium balance and less by arterial stiffness. β(2)M levels were positively associated with insulin resistance. Uremic acidosis may contribute to arterial stiffness.
Abstract: Correlation of coronary artery calcification with pre-hemodialysis bicarbonate levels in patients on hemodialysis.
Coronary artery calcification (CAC) leads to a significant increase in cardiovascular morbidity and mortality in hemodialysis (HD) patients. Metabolic acidosis, which is common in HD patients, promotes bone resorption in human and animals as a result of buffer function of bone, and calcium and phosphate elute from bone into blood stream. However, the effect of acidosis on CAC in HD patients has never been precisely investigated. This is a cross-sectional observational study performed in a single center. One hundred and seven prevalent HD patients (35 women and 72 men) underwent electron-beam computed tomography (EBCT) to evaluate CAC score (CACS), and then we evaluated associated factors of CACS with clinical and laboratory parameters including pre-HD pH and bicarbonate levels. Pre-HD pH and bicarbonate levels were 7.35 ± 0.04, and 17.6 ± 1.8 mmol/L, respectively. The pre-HD pH had no significant correlation to CACS (r = -0.025, P = 0.81). CACS was significantly negatively correlated with pre-HD bicarbonate levels (r = -0.329, P = 0.0009) and serum albumin levels (r = -0.298, P = 0.0467), while it was positively correlated with age (r = 0.319, P = 0.0008) and HD duration (r = 0.385, P = 0.0004). Serum levels of calcium, phosphorus, intact parathyroid hormone, and use of phosphorus binders were not related to CACS. Multivariate analysis indicated that plasma pre-HD bicarbonate level was independently associated with CACS. The present study showed that blood levels of pre-HD bicarbonate were significantly associated with CAC in HD patients. Further studies are needed to confirm these results and to determine whether correction of metabolic acidosis prevents the development of CAC, one of the features of accelerated atherosclerosis in HD patients.
Abstract: Inflammation and arterial stiffness in humans
Arterial stiffness is an established marker of cardiovascular morbidity and mortality and a potential therapeutic target. While hypertension and aging are established factors contributing to arterial stiffness, the role of inflammation in stiffening of the arteries is less well understood. We summarize existing literature regarding inflammation and arterial stiffness, including a discussion of the potential mechanisms by which inflammation may lead to arterial stiffening and studies assessing: (1) The association between subclinical inflammation and arterial stiffness in the general population; (2) The presence of increased arterial stiffness in primary inflammatory diseases; (3) The effect of anti-inflammatory therapy on arterial stiffness in primary inflammatory disease including the effect of statins; (4) Experimental evidence of immunization-induced arterial stiffening in normal adults. We discuss potential opportunities to assess the impact of anti-inflammatory interventions on arterial stiffness in subjects without primary inflammatory conditions. We also review the effect of inflammation on wave reflections.
Bei einer Übersäuerung des Gewebes treten nicht sofort typische Beschwerden auf. Vielmehr ist die Symptomatik unspezifisch und kann oft nicht als eigenständiges Krankheitsbild diagnostiziert werden. Erst im Laufe der Zeit, wenn die Übersäuerung der Gewebe chronisch ist, entstehen 'harte' eigenständige Krankheitsbilder, die dann zwingend mit Medikamenten behandelt werden müssen.
So lange die
Nieren
einwandfrei arbeiten, wird der Säure-Basen-Haushalt im Gleichgewicht gehalten. Bei
Nierenschwäche,
sollten allerdings Medikamente, wie reines magensaftresistentes Bicarbonat, verordnet werden. Diese Arzneimittel werden von den Krankenkassen erstattet, während Nahrungsergänzungen und diätetische Lebensmittel nicht erstattungsfähig sind.


 Mehr zum Sterberisiko bei chronischer metabolischer Azidose können Sie in der folgenden wissenschaftlichen Ausarbeitung lesen. Hier haben wir eine aktuelle Studie ausgewertet, die das Risiko für kardiovaskuläre Ereignisse, wie z. B. Herzinfarkt, Schlaganfall, Herzinsuffizienz, genau quantifiziert.
Mehr zum Sterberisiko bei chronischer metabolischer Azidose können Sie in der folgenden wissenschaftlichen Ausarbeitung lesen. Hier haben wir eine aktuelle Studie ausgewertet, die das Risiko für kardiovaskuläre Ereignisse, wie z. B. Herzinfarkt, Schlaganfall, Herzinsuffizienz, genau quantifiziert.









